


Tomorrow, August 4, 2017, I will return to Mass General Hospital for the second stem cell transplant. I am not ready; I want more time to rest and eat good (nonhospital) food to be “normal.” I don’t want to be inside for 2+ weeks, confined to a hospital floor, gazing longingly out of the windows, trying to imagine what the day feels like from a room that is kept at a constant temperature. In the back of my mind is the repetitive voice of reason explaining how this is needed and how “it’ll be over soon!” etc.
My beard is starting to grow again; it is darker and thicker in some areas and others, just thin indications of hair, translucent almost. Once more, I am surprised at how fast cellular regeneration occurs within the body and, as before, how willing it (the body) is to keep going and growing despite the near-constant bombardment of chemicals. I feel bad that, from tomorrow onward, my body will be fed these toxic chemicals and again will shed the newly grown hairs as the (chemo) agents destroy cells — both good and bad — all cells.
Again, the voice tells me it is for the best, this is about healing, “you’ll be well soon,”… etc.
When I was just a small child, I played in the woods near our house. For some reason, I consumed some berries growing wildly in the forest. As innocent as a child is, I just thought they were harmless and would taste yummy. When my mother heard it, she immediately called the doctor, who had the pharmacist deliver (yes, they delivered!) ipecac syrup. This is used to induce vomiting and administered if something potentially poisonous is ingested. Since my mother didn’t know what type of berries I had feasted upon, she assumed the worst. Naturally, she felt horrible when I vomited up what I could barely remember as a colorful, Pollock-like splatter of colorful berries (amongst other things recently consumed). I now feel the way my mother must have when she was trying to explain to me why I would feel poorly – and that it was for my safety – and that she was sorry – and that she loved me.
At night, or when first waking, I scan my body mentally from head to toe and envision myself embracing my own body as I explain why this must be endured – and that I’m sorry – and that I love it.

I checked into Mass General today for what will be 1 of 2 stem cell transplants.
This will be a long summer & the realization of what I’m in for struck me when I started unpacking and settling in.

I spent the last five days in the hospital. During this time, I was receiving a continuous flow of IV antibiotics in an attempt to nip whatever was lurking in the bud to stay on track with an MGH/stem cell transplant. This didn’t go as planned when the fever spiked, and I missed the stem cell collection scheduled for Wednesday.
That afternoon (on Wednesday), while still hospitalized in Maine, the oncologist whose care I’m currently in at MGH called me. At this point, it seemed apparent that my fever was a result of neutropenia as well as from the filgrastim injections ( http://www.neupogenhcp.com/).
The blood drawn for cultures hadn’t, after 48 hours, indicated a blood-borne infection. The oncologist at MGH was convincing & practically demanded that I get discharged, drive down to Boston that afternoon/evening, and make the 07:00 Stem cell collection already on the books for the following day (Thursday, June 8). to me, this sounded reckless. I didn’t want to be in the hospital longer than needed, but I also was fearful of the big, germ-filled world waiting to sneeze on me and send me back to the ER. I feared that, should this happen, should my fever spike force me to the hospital for another 5 days or more, this would further delay the actual transplant. (something that has been postponed already due to cancer-related issues!) his fear was a different side of postponement & delay – that the small window of opportunity after the nadir (which refers to the lowest point that an individual’s blood cell count
will reach as a side effect of chemotherapy) & the peak reached as a result of the injections, would close on us. He was worried that if I didn’t make it Thursday to collect and thus left only Friday, we were taking a massive gamble as most people need at least two days to collect all the stem cells they will need for a transplant. If I were to wait until Friday and NOT gather all the cells, we’d have to finish on Monday and hope the injections were still assisting in generating the needed stem cells. It’s not only the shots that assist in this generation of cells! The whole reason for undergoing the monstrous round of chemo/etoposide was to send the body (after nadir) into white blood cell count overdrive! Add daily shots to the mix to assist this, and boom – massive (daily, maybe hourly?) jumps in cell counts.
So what did I do? I got discharged (June 7) and made the trip to Boston.
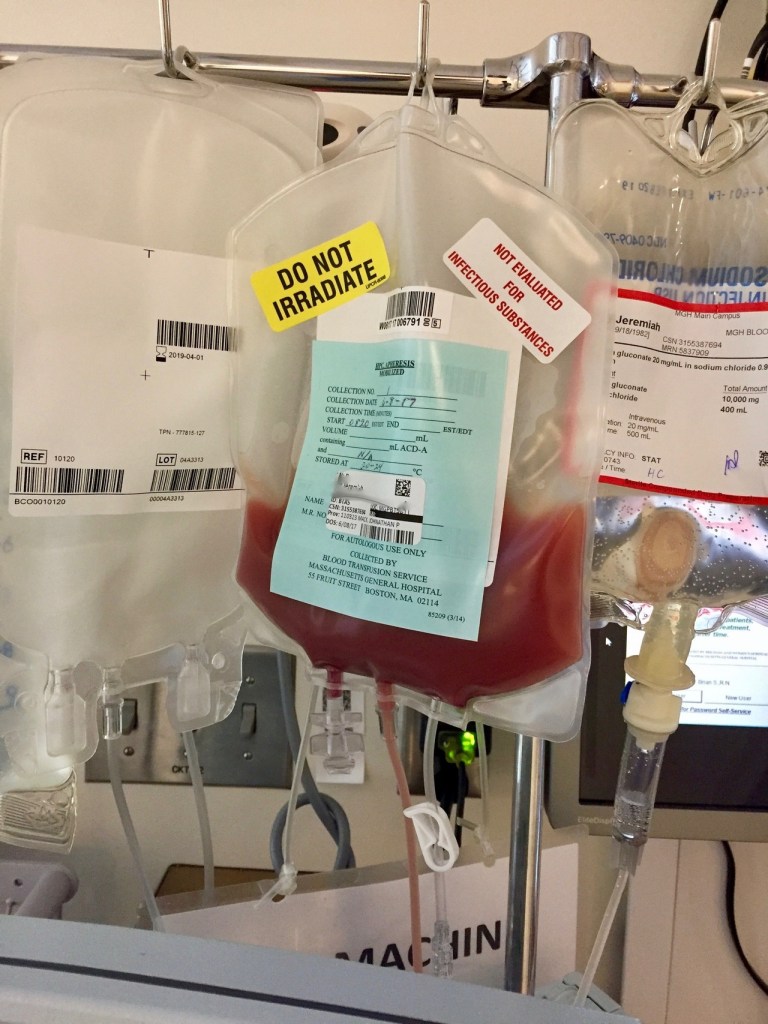
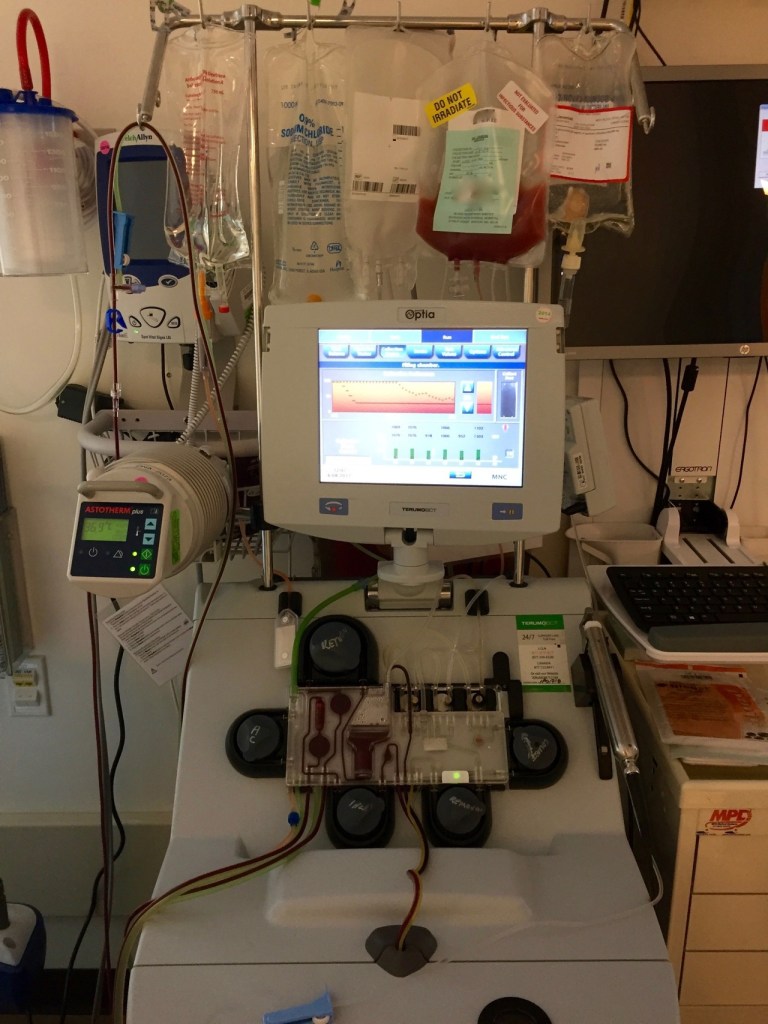
Today, June 8 (2017), at 07:00, I walked over to Mass General Hospital for collection. The process took several hours. My triple lumen pheresis catheter (seen in photos, the line coming out of my chest) worked perfectly!
When I was finally free, I took a much-needed stroll around the area to get fresh air and sunlight. I was awaiting a call from the nurse practitioner to tell me whether or not the collection was successful or if I needed to return the next day to finish up.
The plan worked, and, though one day off schedule, they gathered all the cells needed in one session.

I should know this by now, but I don’t’; things change very quickly– alarmingly so.
The other day, I noticed that typing with my left hand was challenging. It wasn’t easy to access specific keys. Later that day, when attempting to play guitar, I again noticed that the fluidity with which I usually fingered the chords (using my left hand) wasn’t present.
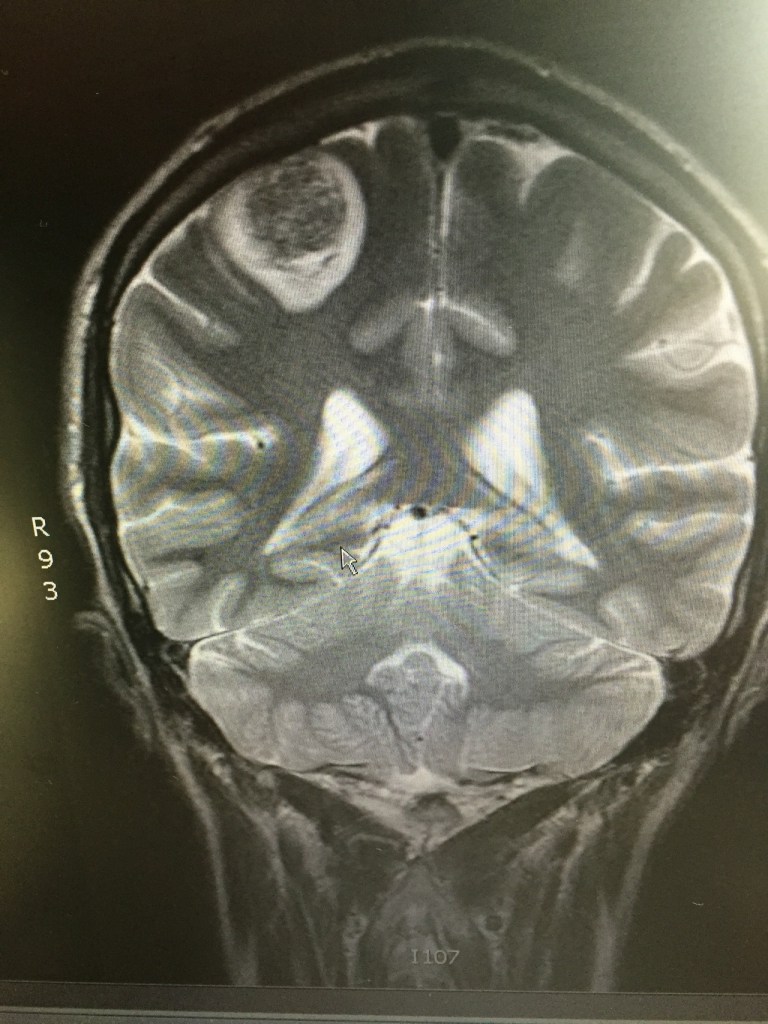
The following day, while driving back from an appointment, I lost complete mobility in my left arm. Unsure if this was a seizure, a stroke…, or a clotting issue, my sister took me to the ER. As most of my ER stories go, they did several tests, the first of which, after vitals, was a head CT scan. What they discovered explained the loss of mobility/motor function in my left arm – a 3.2cm lesion on the back rear (right) lobe in and around the parietal and occipital lobe. (this is what I’m piecing together from the various doctors I’ve met. still trying to grasp the facts.) My MRI on Jan 30 showed no sign of this (what is assumed to be) metastatic spread. Unlike the other brain lesion that was dealt with using solely stereotactic radiosurgery (SRS) in early October (2016), this one will initially be surgically resectioned, and then SRS will be used. The main reason for that is its size.
This will most likely push back the stem cell transplant a few weeks or so, considering the healing time and then the radiation therapy afterward. That & this new and particularly aggressive/fast-growing brain met seem most urgent.
The surgical resection is scheduled for tomorrow, Apr 30, 2017.

This fun-looking piece of facial equipment & headgear is not for a new sport but rather to keep my head entirely immobile while the procedure (stereotactic radiation, or SRS) is being performed. This fashionable piece was constructed a few weeks ago when I went down to have an updated MRI (used for planning the procedure), to have a “bite-block” (dental mold) constructed, along with a fancy, net-like structure that was formed to the back of my head. … Then, this elaborate gadget, which I’m sure was used during (the) inquisition, was bolted to the table.
