Where and how do I begin explaining high-dose chemotherapy with (tandem) stem cell transplants? I have been considering how I should go about describing the process. However, I wasn’t even sure I understood it correctly.
In my case, and this might be the same for other patients, I am not sure, but upon admittance, the clock starts at “day -5” (day negative 5). so “day 0” is when I return my stem cells. Days -5 — 0 are, as you might have guessed, chemo days. By this, I don’t mean normal outpatient days that, in my case, lasted several hours, depending on the regimen. No, I am talking about round-the-clock infusions, IV bags of chemotherapy drugs that run for 24 hours and then are switched out for new bags that run the same length for days and days. The intention, with such long days filled with heavy-duty chemo, is to destroy the current stem cells/marrow & annihilate the existing cancer and then replenish my system with untouched (by high dose chemo) stem cells from which my body will reconstruct itself literally from the ground up.
Along with the continuous stream of chemo, I have also been receiving liters upon liters of fluids. This is to prevent any damage to the liver, kidney & bladder. However, it is often uncomfortable, and, according to the nurse, I am currently retaining 8lbs/3.6kg of excess liquid. Needless to say, I feel uncomfortably bloated.
Between days -2 and 0, I will just be receiving mesna, a chemo protectant, and more fluids to continue to flush my filter organs.
I should know this by now, but I don’t’; things change very quickly– alarmingly so.
The other day, I noticed that typing with my left hand was challenging. It wasn’t easy to access specific keys. Later that day, when attempting to play guitar, I again noticed that the fluidity with which I usually fingered the chords (using my left hand) wasn’t present.
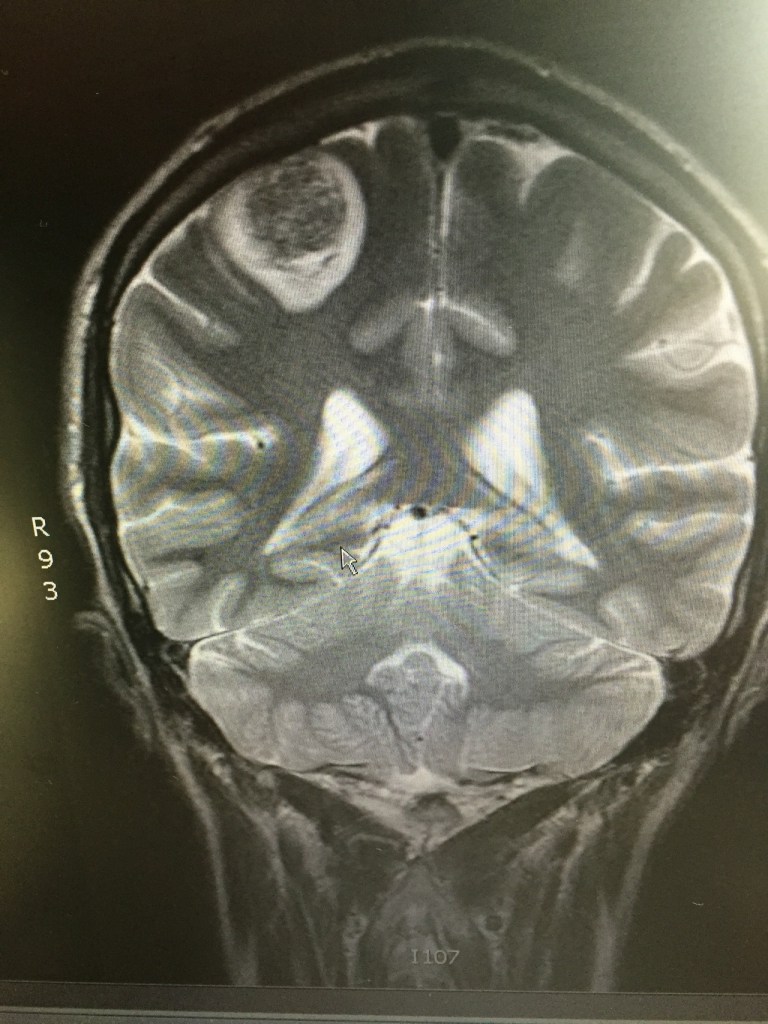
The following day, while driving back from an appointment, I lost complete mobility in my left arm. Unsure if this was a seizure, a stroke…, or a clotting issue, my sister took me to the ER. As most of my ER stories go, they did several tests, the first of which, after vitals, was a head CT scan. What they discovered explained the loss of mobility/motor function in my left arm – a 3.2cm lesion on the back rear (right) lobe in and around the parietal and occipital lobe. (this is what I’m piecing together from the various doctors I’ve met. still trying to grasp the facts.) My MRI on Jan 30 showed no sign of this (what is assumed to be) metastatic spread. Unlike the other brain lesion that was dealt with using solely stereotactic radiosurgery (SRS) in early October (2016), this one will initially be surgically resectioned, and then SRS will be used. The main reason for that is its size.
This will most likely push back the stem cell transplant a few weeks or so, considering the healing time and then the radiation therapy afterward. That & this new and particularly aggressive/fast-growing brain met seem most urgent.
The surgical resection is scheduled for tomorrow, Apr 30, 2017.
To me, a stem cell transplant is still a mystery. I understand it theoretically, but it still seems like some sorcery. When I spoke briefly via phone with the doctor in charge of bone marrow/stem cell transplants at Mass General Hospital (MGH) before my appointment (April 20), it sounded like he wanted me to start the procedure the following day. There was this sense of urgency. I was, and am, ready. I needed the time (since being told of the recurrence) to accept and come to terms with it and thus prepare myself (on every level) for the next steps. Being “ready” on a purely medical level is accepting what is and the facts. Being “ready” on every other level only acknowledges the work and tasks ahead.
When initially diagnosed, I didn’t have time to think about everything, seek out other opinions, or talk to survivors and current patients in treatment. It was a seizure, hospitalization, surgery, and treatment. I understand that some of me was in denial when informed of the recurrence. Naturally. I also knew, from the crash courses I had given myself in oncology & cancer treatment (etc.), that, this time, I did have some time. As aggressive as my cancer may be, I knew I owed it to myself (and my body/mind!) to seek advice. Since all signs keep pointing back to this route, that of high-dose chemo with tandem stem cell transplants, I feel a sense of readiness. Also, and most importantly, I needed the time from my meeting with my oncologist (February 2) until I met with Dr. Einhorn (April 5) to not only research and explore but also cry, scream, and walk in circles in the woods (literally) to grasp it. In doing so, I unblocked and addressed some of which I didn’t have time to deal with initially when I was first diagnosed. Looking back, I am thankful for this time. Not only did I get to explore and look into the vast world of alternative therapies (clinical trials, studies, etc.). But I also had the pleasure of meeting (by phone, e-mail, or in person) some beautiful folks. On top of this, and perhaps most importantly, I got a better look at some of the emotions I “didn’t have time” to address before.
Anyways… those next steps, the preparatory stages, are even more complex than the (stem cell transplant) procedure itself, or so it seems. I suppose this makes sense, being that the very nature of a stem cell transplant (2 transplants in all) is so involved and brutal on the body that there needs to be adequate preparation. It’s not just relatively basic and seemingly simple stuff, like having my dentist sign off stating that any routine work has been done in their professional opinion is that my teeth are fine and ready, etc. It’s more timing and lining everything up so that it all is methodically prepped and in place that, like clockwork, it follows a pre-determined, pre-planned, pre-mediated schedule with such exactitude. I’ll break it down by posting updates as things move along.
Right now, the plan is to receive a single infusion of Etoposide on May
5th. Etoposide is a chemotherapy drug. I received it in various regimens during my initial treatment. The idea behind a single, stand-alone dose is to push the body into generating white blood cells to initiate a sort of overdrive in production. This is the body’s natural response under normal conditions while undergoing conventional chemo. Even though etoposide has cancer treatment and maintenance “benefits,” we’re using it to jump-start white blood cell production. After a two-day pause, just after the etoposide has flushed from my system and right when my body is in white blood) cell production, I will start giving myself daily white blood cell booster injections. I had these before; however, this was after the week of cisplatin-based therapy when my white blood cell was deficient & dangerously so. After 10 days of forcing my marrow into overdrive production, I’ll go in for harvesting.
Before high-dose chemo, which destroys my marrow, harvesting is done so there are adequate platelets to replenish that which is killed off by the high dose of chemotherapy.
Currently, all of these procedures will be done at MGH. I won’t be inpatient until I start high-dose chemo, as this will require a sterile, germ-proof environment.
This fun-looking piece of facial equipment & headgear is not for a new sport but rather to keep my head entirely immobile while the procedure (stereotactic radiation, or SRS) is being performed. This fashionable piece was constructed a few weeks ago when I went down to have an updated MRI (used for planning the procedure), to have a “bite-block” (dental mold) constructed, along with a fancy, net-like structure that was formed to the back of my head. … Then, this elaborate gadget, which I’m sure was used during (the) inquisition, was bolted to the table.